Welcome back to my dissection of the Fast Track Trial paper ‘Symptoms of Depression, Eating Disorders and Depression in Adolescents With Obesity‘. This will make much more sense if you read Part 1 first. A heads up – this post contains multiple references to fat phobic language and explicit discussion of eating disorder symptoms, so please take care.
In my last post we covered the results of the Fast Track’s ‘screening and monitoring’ for eating disorder risk. It’s more accurate to say we uncovered the lack of data presented, leaving us with more questions than answers.
Speaking of which, I’ve had no answers to the 25 questions sent to the lead author Dr Hiba Jebeile, who has been busy accepting a ‘Young Investigator of the Year Award’ at a Novo Nordisk sponsored obesity conference.
|
|
Fast Track To The Diet Trap
Although not discussed in their paper, the Fast Track data demonstrated a well known fact about food restriction – it produces a temporary ‘white knuckling’ period during which people use willpower to stop themselves from eating, but as time progresses this becomes extraordinarily difficult to sustain. Before too long, people ‘give in’, and behaviours such as binge eating, over eating, or feeling out of control return. This isn’t a ‘failure of willpower’ – it’s a natural response to restriction. I call it the Diet Trap.
We can literally see the diet trap cycle playing out in the Fast Track teens’ overeating, loss of control eating, and binge eating behaviours:
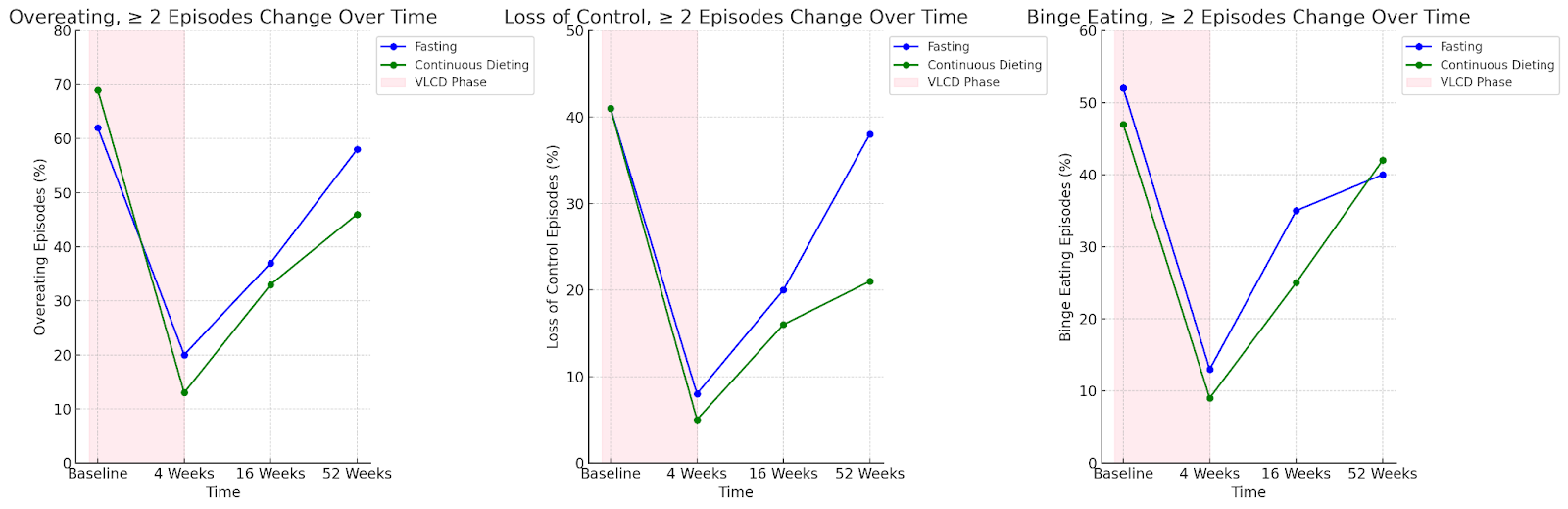 |
There’s a big drop during the first 4 weeks when the kids were on the milkshakes, but one year later we see a massive rebound. Worryingly, the fasting group showed a stronger rebound compared to the continuous diet group, especially with ‘loss of control’ eating.
Incredibly, the Fast Track paper didn’t discuss this at all. Given that they were allegedly interested in how:
‘self-reported symptoms of depression, eating disorders, and binge eating change for adolescents with obesity during an intensive behavioral intervention?’ (emphasis added)
…the decision to exclude such important information is worrisome.
A rebound pattern also happened for ‘dietary restraint,’ a sub scale of the Eating Disorder Questionnaire (EDE-Q) which measures the cognitive effort to restrict eating. Dietary restraint is literally a measure of ‘willpower’. Here’s what happened to the Fast Track teens’s dietary restraint over time (I’ve illustrated this alongside the BMI rebound data):
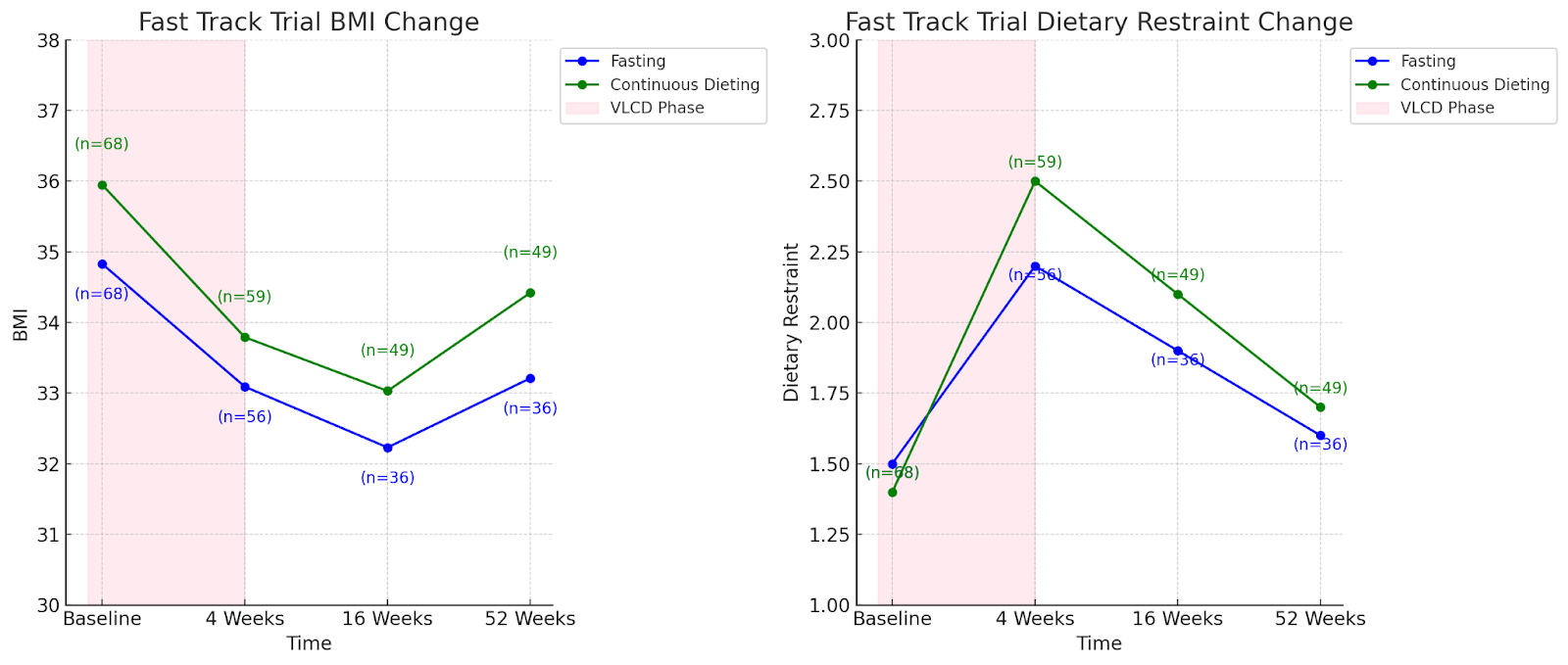 |
As we can see from the graph on the right, a spike in dietary restraint during the 4 week milkshake phase was followed by a drop almost to baseline at 1 year. This unravelling of willpower matches the data for overeating, loss of control and binge eating, and the weight regain trend. We’re seeing just how hard it is to sustain restriction. The diet trap is literally playing out in front of us, just as it has in more than 70 years of weight loss research.
But in a truly ham fisted argument the Fast Trackers claimed that the reduction in dietary restraint scores was because:
‘dietary prescription in the context of a multidisciplinary care poses less risk than when undertaken without supervision in the community. We speculate that this is due to the multidisciplinary nature of the intervention and frequency of support provided by trained clinicians.’ (emphasis added)
|
|
This speculation is a red herring, completely irrelevant to the actual findings. Lacking a control group of teens dieting ‘without supervision in the community,’ no claims should be made about the alleged superiority of their team. Congratulating themselves for ‘safely’ reducing dietary restraint, whilst ignoring their own evidence that it reduced because the kids just couldn’t sustain strict dieting, is simply unhinged.
Yet unhinged claims are typical for the Fast Track team, who habitually ignore the most likely evidence based explanations in favour of those fitting their narrative.
Eating Disorder And Depression Outcomes
It’s unclear why the researchers chose to pair these particular issues into one paper, separated from weight and other mental health outcomes. Data from 3 self-report measures – the Eating Disorder Questionnaire – (EDE-Q), the Binge Eating Scale (BES), and a 10 item depression measure (CEDR-10) – are presented. Although 97 kids completed the Fast Track, eating disorder and depression score data was only presented for 92, with no explanation offered. And although teens completed two other relevant measures of eating disorder and depression symptoms (the Depression, Anxiety & Stress, or DASS scale, and the Dutch Eating Behaviour Questionnaire, or DEBQ), results for those measures appear in a separate, (as yet unpublished) paper, once again without explanation.
McNuggets
I have issues with the extent to which these results have been sliced and diced into a series of publications. There’s clear career advantages for ambitious, award-winning Fast Track researchers to rack up their publication count, but discombobulated snippets do a great disservice to science. The information is decontextualised, the bigger picture obscured. There’s no way, for example, for us to understand the relationship between weight fluctuations and the teens’ mental health. It’s a McNugget of information, when we need the whole chicken.
|
|
The Fast Track trial was funded by $1.2 million of public research money, yet they are refusing to share the data. When researchers use tax payer funds, the anonymised data should be publicly available. Not only does data sharing ensure research integrity, allowing for much needed checks and balances – it’s basic good manners.
Eating Disorder Risk Outcomes
Scores above 2.7 on the EDE-Q indicate clinically elevated eating disorder symptoms. At baseline the average EDE-Q score was 2.4 for the Fasting group and 2.3 for the Continuous Dieters. 4 weeks later – after the kids lost an average of 5.5kg during the Optifast milkshake stage – this reduced to an average of 1.7 for the Fasting group and 1.9 for the Continuous Dieters.
How on earth would going on a strict diet reduce average eating disorder scores, and so quickly, I hear you ask? The Fast Trackers don’t interrogate this, flippantly stating:
‘It is possible that the initial reduction in BMI, together with frequent support, improved mental well-being’.
Much of the distress captured by the EDE-Q reflects the person’s desire to become smaller, so this quick reduction reflects the person’s belief that they’re on the way to being thin. This correlation with initial (and temporary) weight loss is concerning, not encouraging.
As an eating disorder therapist it’s fascinating (and horrifying) to see these EDE-Q averages, but not for a hot minute am I convinced that teen eating disorder symptoms can be ‘cured’ by weight loss. Imagine if extreme diets were recommended to people with low-BMI eating disorders?!
Eating Disorder Symptoms: Risk Vs Benefit?
Digging more deeply into the EDE-Q results, of 92 kids, 25 (27%) improved, changing from above the clinical cutoff of 2.7 to below it. The extent to which these improvements were related to weight change wasn’t reported (yet another data-hole in this paper).
|
|
But 16 kids (17%) either developed new EDE-Q elevations or remained clinically unwell with scores >2.7. As I said in Part 1, kids remaining unwell during a year long starvation trial is unacceptable.
8 kids (9%) who scored normally at the beginning developed clinically relevant eating disorder scores, direct evidence that the Fast Track’s prolonged restriction produced harm. Yet the researchers don’t even mention this as a possibility.
Instead they blame ‘psychological comorbidity.’ But this is another red herring: only half the teens who developed clinically elevated EDE-Q scores were flagged at baseline. This proves once again that the Fast Trackers’ careful screening and monitoring was as accurate as flipping a coin when it came to identifying allegedly ‘at risk’ teens, and demonstrates that strict diets can cause clinically elevated eating disorder scores even in adolescents without pre-existing psychological issues.
Binge Eating Results
For reasons unexplained, only 135 kids completed the BES at baseline, leaving 6 unaccounted for. On average, binge eating scores were not clinically elevated to begin with. After 4 weeks on the liquid diet, scores were significantly reduced for both groups, but at 1 year the Continuous Dieting group spiked back up while the Fasting group’s scores remained suppressed. As an eating disorders therapist, this isn’t surprising to me – people undertaking more extreme diet regimes can show a more ‘on/off’ extreme pattern – they’re likely white knuckling that willpower!
Binge Eating Results: Risk Vs Benefit?
A closer look through the binge eating data reveals a concerning picture. At baseline 23 kids scored ‘mild to moderate’ binge eating and 5 scored ‘severe’. From the 92 who stayed til the end, 12 (13%) with elevated binge eating scores improved, but this was completely overshadowed by 15 (17%) who either stayed unwell (5, 5%) or worsened (10, 11%).
|
|
Overall, the Fast Track trial left more kids worse off than improved for binge eating. The researchers admitted that 10 kids experienced worsening binging, but rather than identifying the strict diet as the cause they revert to blaming ‘mental health conditions,’ although again only half had such ‘conditions’.
Depression Results
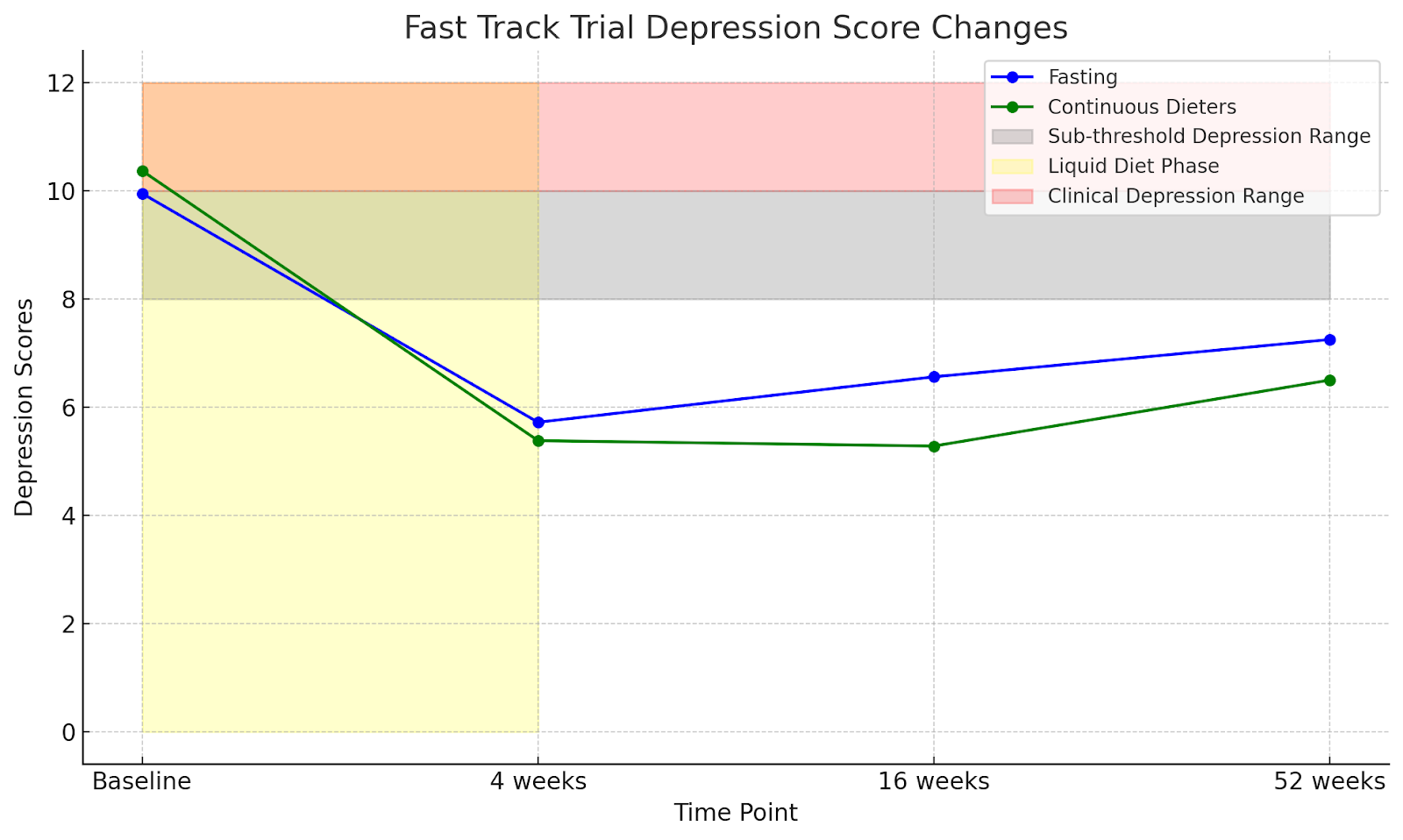
A score >8 on the CEDR-10 indicates subthreshold depression, and scores higher than 10 indicate ‘possible, probable or major depression in the last week’. At baseline, 55% of the teens scored 8 and above, and by 52 weeks 35% of the remaining 92 had scores >8. We’re not told how the trials’ 30% drop out rate impacted these figures.
Depression score improvements mostly happened over the first 4 weeks – when the kids were losing the most weight. By week 52 there’s a clear trend back up, with both groups nudging the sub threshold range.
 |
Depression: Risk Vs Benefit?
I can’t present risk vs. benefit for depression scores, because for unexplained reasons the paper didn’t report the number of teens improving from scores above the threshold to below, or how many teens remained unwell over the course of the trial. They only reported those who worsened: 5 teens – 5% – with no elevations at baseline moved to either sub-threshold (4) or probable (1) depression. Continuing their theme of blaming pre-existing mental health issues instead of the diets, the Fast Trackers reported the person with probable depression had a ‘history of long standing depression’. We’re not told if this person had been flagged and offered support at baseline, and presumably the other 4 did not have pre-existing problems: the diet itself was enough to trigger worsening mood.
Starving Teenagers: Risk Vs Benefits
In weight centric research, the risks involved in weight loss interventions are often claimed to be ‘worth it’ because of the anticipated benefits. The Fast Track trial’s consent form told potential participants and parents that:
‘We do not expect any significant side effects or risks associated with this study…It has been suggested that exposure to restrictive dieting may increase the risk of eating disorders. However, it is considered that this potential risk is minimal and manageable.’
So was the risk minimal and manageable? Sadly we can’t answer this by reading the article, because it didn’t provide a risk vs benefit analysis, they only state that:
‘few adolescents had increased symptoms during the trial’.
Risk vs benefit is an important topic which deserves more accuracy than ‘few’. I crunched the numbers and found that for combined EDE-Q and BES score results, 63% of the Fast Track teens remained below clinical levels throughout. 20% of kids who began the trial with clinically elevated scores reduced to a nonclinical level. But 10% developed new eating disorder symptoms, and 7% remained unwell.
As a comparison, my previous number crunching of their meta-analysis revealed rates of kids experiencing disordered eating after ‘professionally supervised’ weight loss programs between 5-9%, and this was in studies with >2 year follow ups. The Fast Track results – 17% either remaining unwell or developing new disordered eating after only 52 weeks – are alarmingly high.
What’s the point of ‘curing’ 20% of teens only to create or prolong the same problems in another 17%? This experiment has created a revolving door of diet-cycle misery. They’ve literally created a Fast Track to the Diet Trap.
|
|
The kids whose scores improved are simply white knuckling restriction, while the ones staying unwell or developing disordered eating are in the ‘bust’ phase of the diet trap.
Quantifying risks vs benefit has revealed an unacceptably high risk level of 17%, and this doesn’t include the 5% of the teens with worsening depression. Risk is further underestimated as 30% of the teens dropped out early, and an unknown proportion of them could have experienced harm.
Let’s also consider the Fast Track casualties:
- one teen battling diet-induced Atypical Anorexia (AAN)
- one in therapy for self esteem & body image problems
- one without a gallbladder
All of this for a temporary 5kg weight loss. Does this risk/benefit profile seem worth it to you?
|
|
Yet the paper confidently concludes:
‘Overall, participation in intensive behavioral interventions using a prescriptive dietary approach did not worsen mental health or eating behaviors. Indeed, an improvement in self-report symptoms was seen.’
Such glib erasure of the harm wreaked by the Fast Track Trial makes me so mad I could scream. This team’s refusal to present proper risk analysis or acknowledge the role their strict diet regime played in the development or prolonging of disordered eating in 17% of their kids is astounding. This is not science, it’s self-serving propaganda, and these researchers (and their peer reviewers) need to be held to account.
I’m not done yet. Stay tuned for an upcoming episode of the All Fired Up podcast, where I’ll get it all off my chest – and share the incredibly gaslighty experience that was the Fast Track webinar!
Please share my Fast Track Trial series with everyone you can – I want to get the word out to as many people as possible.
Thanks for reading my rant,
Louise x
If you are struggling with issues relating to food, your body, exercise, or with an eating disorder, I can help (no fasting required!). I have offices at Flourish Kirribilli, in Sydney, and am also available for online appointments. If you’re a health professional looking for hep with providing weight-inclusive care I also provide clinical supervision, and my books are currently open.